|
 Overview | Understanding Coagulation | Assessment & Monitoring | Clinical Contexts | Treatment Strategies | Reversal of Anticoagulation & Antiplatelets | Guidelines & Evidence Overview | Understanding Coagulation | Assessment & Monitoring | Clinical Contexts | Treatment Strategies | Reversal of Anticoagulation & Antiplatelets | Guidelines & Evidence
Pharmacologic Alternatives: Antifibrinolytics
Contributed by: Prakash A. Patel, MD, FASE

The fibrinolytic system is a necessary component of our hemostatic mechanism which is required to maintain vascular patency. Fibrinolysis remains in balance with coagulation to prevent excessive clot growth by breaking down fibrin. This process first involves the activation of plasminogen (produced in the liver) to plasmin by tissue plasminogen activator (released from injured tissues). Plasmin can then act directly on fibrin to break it down into fibrin degradation products.1 The balance between coagulation and fibrinolysis can shift towards excessive fibrinolysis after certain situations such as trauma or surgery, resulting in excessive bleeding.
Fortunately, there are strategies to manage excessive fibrinolysis and the associated bleeding. Pharmacologic agents can be given preemptively to prevent or decrease fibrinolysis. These include antifibrinolytic agents, which happen to be the most extensively studied blood conservation agents. Their value in decreasing bleeding and allogeneic transfusion requirements has been well demonstrated across a wide range of clinical settings.1,2 Aprotinin, a serine protease inhibitor, was once highly utilized for both its’ antifibrinolytic and anti-inflammatory properties, but safety concerns including increased mortality led to aprotinin’s withdrawal from clinical use.3 Although limited re-introduction of aprotinin in Canada and Europe had taken place for select high-risk cases, ongoing uncertainty about the value of aprotinin will limit the remainder of our discussion to the currently available lysine analogue antifibrinolytic agents: epsilon-aminocaproic acid (EACA) and tranexamic acid (TXA) (Figure 1).4
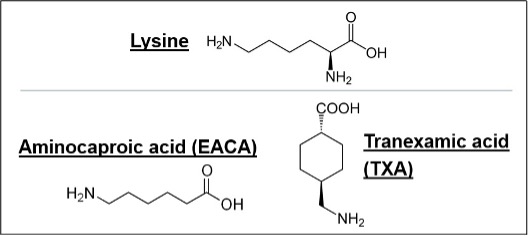
Figure 1. Structural similarity of EACA and TXA to the amino acid lysine.
TXA: tranexamic acid; EACA: epsilon aminocaproic acid.
Lysine Analogues
The role of lysine analogue agents in preventing fibrinolysis is based on their ability to competitively bind to lysine-binding sites on plasminogen. When bound to either EACA or TXA, plasminogen is unable to bind to fibrin; therefore, preventing its’ activation to plasmin (Figure 2).1 While the mechanism of action for both EACA and TXA is similar, the potency of TXA is often reported as being as high as 10 times greater based on molecular concentration.5 Despite the greater potency, direct comparisons of TXA and EACA, especially in cardiac surgery, have not consistently demonstrated a clinically relevant difference as far as decreased bleeding or need for transfusion.5,6 However, TXA continues to be more extensively investigated when compared to EACA due to its greater global availability, widespread access, and off-label uses.1 The positive impact of TXA on patient outcomes has even landed it on the World Health Organization’s List of Essential Medicines.7 As far as safety concerns, TXA has been associated with a dose-dependent increase in the risk of seizures, while limited data has suggested an increased incidence of postoperative renal failure with EACA.5,8,9
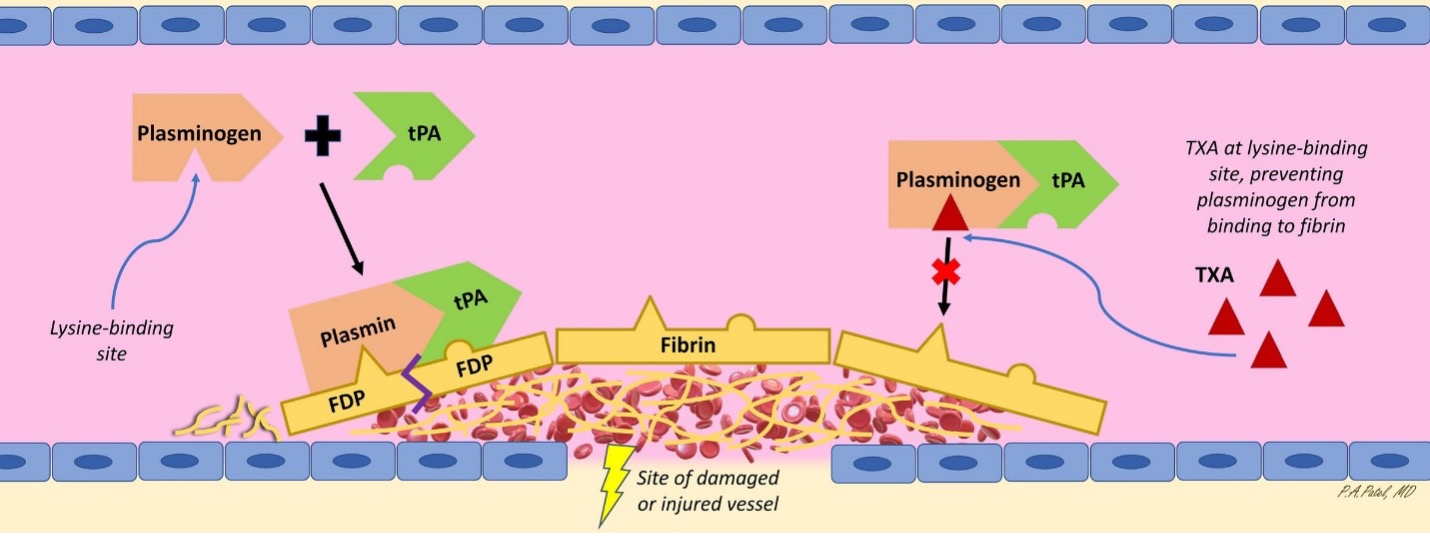
Figure 2. Fibrinolysis occurs when plasmin degrades the fibrin within a clot into FDPs. However, in the presence of a lysine analogue antifibrinolytic, competitive binding at the lysine-binding site on plasminogen prevents plasminogen’s activation to plasmin. (EACA would act at same site as TXA shown in figure.) FDP: fibrin degradation product; tPA: tissue plasminogen activator; TXA: tranexamic acid; EACA: epsilon aminocaproic acid. [Reprinted with permission from Reference #1].
Antifibrinolytics for Cardiac Surgery
Routine use of lysine analogues in cardiac surgery has become the standard of care with strong evidence demonstrating reduced blood loss and a decreased need for allogeneic transfusion. Current blood conservation guidelines give lysine analogue antifibrinolytics a Class 1 A recommendation for use in cardiac surgery.10 Along with cases involving cardiopulmonary bypass, evidence also exists suggesting a benefit in off-pump coronary artery bypass grafting (CABG) without an increase in the incidence of prothrombotic events.11 The landmark ATACAS trial demonstrated superiority of TXA over placebo in decreasing transfusion and re-exploration in CABG patients without impacting graft patency.8 Despite the abundance of well-established data, several concerns remain regarding the use of antifibrinolytics in cardiac surgery. Optimal dosing continues to be investigated. Currently, there is significant variability among institutions for loading doses and infusion rates for both EACA and TXA. While obtaining a target plasma concentration can be achieved with various dosing strategies, recent investigations into of pharmacokinetic models using glomerular filtration rate and plasma clearance may help guide dosing without leading to excessive plasma concentrations.12 Determining optimal dosing may also lead to decreased adverse events. As noted in a 2019 meta-analysis of over 10,000 cardiac surgery patients, high-dose TXA regimens (≥50 mg/kg bolus only or >10 mg/kg bolus + infusion) resulted in a 4.83 times greater risk of seizures when compared to a low-dose TXA regimen (<50 mg/kg bolus only or ≤10 mg/kg bolus + infusion). Both groups had similar efficacy in terms of decreasing transfusion requirements.13 However, a more recent randomized trial of low-dose (10 mg/kg bolus + 2 mg/kg/hr) and high-dose (30 mg/kg bolus + 16 mg/kg/hr) TXA strategies in cardiac surgery found superiority with the high-dose regimen in decreasing allogeneic red blood cell transfusion, while also showing no difference in a composite safety endpoint that included the incidence of seizures.14 Given these conflicting findings, further studies are still warranted despite the well-established benefits of antifibrinolytics in cardiac surgery.
Antifibrinolytics for Trauma
Trauma-induced coagulopathy is the result of multiple causes including fibrinolysis. Therefore, antifibrinolytic therapy remains a critical component in the treatment of trauma-induced coagulopathy.1 Given TXA’s faster onset of action over EACA, the vast majority of evidence for antifibrinolytics in trauma comes from TXA. While there is strong evidence for the use of TXA in select trauma patients, we are learning more about the dynamic nature of fibrinolysis where changes after initial injury may result in hyperfibrinolysis or hypofibrinolysis.1 This is consistent with the findings of the 2010 CRASH-2 study that demonstrated decreased all-cause mortality and decreased risk of death due to bleeding in only those patients who received TXA within 3 hours of injury (greatest benefit when within 1 hour of injury).15,16 Retrospective military data used in the MATTERs trial also found a similar mortality benefit with TXA.17 Given the benefits of early TXA administration, a meta-analysis of prehospital TXA use was conducted and found that 24-hour mortality was significantly reduced with prehospital TXA compared to no TXA.18 The same analysis also found no differences in thrombotic events. However, more recently, the value of prehospital TXA has come into question as 6-month survival with a favorable functional outcome has not differed when compared to placebo.19 Further work on timing of administration may best be guided by laboratory markers of fibrinolysis or viscoelastic testing.1
Antifibrinolytics for Orthopedics
The utilization of antifibrinolytics in orthopedic surgery is much higher than other non-cardiac surgeries.20 Given the value in decreasing surgical blood loss and decreasing the need for allogeneic transfusion, it is not surprising to see that clinical practice guidelines for total joint arthroplasty have endorsed routine antifibrinolytic use.21 TXA, in particular, has demonstrated efficacy in topical, oral, and intravenous forms in reducing transfusion risk when compared to placebo.22 While most studies again demonstrate the benefit of TXA, EACA has also been effective without an increased risk of adverse events as shown by a meta-analysis of over 750 patients undergoing knee or hip arthroplasty.23 Despite concerns for thromboembolic risk in the orthopedic population due to greater comorbidities including coronary disease and hypercoagulable states, the current evidence would suggest no difference in complication rates with antifibrinolytics. This was recently demonstrated in an analysis comparing joint surgery patients with coronary disease (+/-stents) to those without coronary disease.24 All patients received TXA, and no differences in venous thromboembolism were noted for the groups, again emphasizing that antifibrinolytics are clot stabilizers; not clot producers.
Antifibrinolytics for Obstetrics
In obstetrics, the primary use of antifibrinolytics is for the treatment of postpartum hemorrhage (PPH), which is a leading cause of maternal death and morbidity.1 While uterotonic therapy is given as a first-line agent, addressing uterine atony alone does not treat other potential causes of bleeding such as hyperfibrinolysis.25 An increase in tissue plasminogen activator after removal of the placenta contributes to a highly active fibrinolytic system. TXA has been shown to decrease PPH bleeding, as evidenced by the landmark WOMAN trial.26 In this study, over 20,000 women with PPH from low- and middle-income countries were randomized to TXA or placebo. A significant decrease in the risk of death related to bleeding was seen in the TXA group, specifically when given within 3 hours of birth. Despite concerns that the study’s findings may not be generalizable to more developed countries with well-resourced hospitals, the recommendation for TXA in treating PPH has been widely adopted. More recent investigations into the prophylactic use of TXA for prevention of PPH after vaginal delivery have not resulted in a difference when compared to placebo.27 In Cesarean delivery, similar analyses have only shown a small difference in blood loss between TXA and placebo groups, with no difference in maternal death or transfusion.28,29 Therefore, prophylactic use of TXA for PPH prevention is not typically recommended.
Antifibrinolytics for All Non-cardiac Surgery
With the benefits of antifibrinolytics being well-established in managing fibrinolytic bleeding in several clinical situations, expansion to even more surgical settings continues. Antifibrinolytics now have a role in neurosurgical, spine, craniofacial, vascular, urologic, gynecologic, thoracic, and other surgeries.1,30 The POISE-3 trial investigated the impact of antifibrinolytics, specifically TXA, in over 9000 patients undergoing a variety of non-cardiac surgery.30 Patients were randomized to TXA 1g or placebo. Those receiving TXA experienced a lower composite bleeding outcome at 30 days, but noninferiority in terms of a composite cardiovascular outcome was not demonstrated despite a very small between-group difference. With this continued safety concern, the investigators suggest that clinicians weigh the clear benefit of TXA in noncardiac surgery against the low likelihood of increased risk.30
References
- Patel PA, Wyrobek JA, Butwick AJ, et al. Update on applications and limitations of perioperative tranexamic acid. Anesth Analg 2022;135(2):460-473.
- Levy JH, Koster A, Quinones QJ, et al. Antifibrinolytic therapy and perioperative considerations. Anesthesiology 2018;128(3):657-670.
- Fergusson DA, Hebert PC, Mazer CD, et al. A comparison of aprotinin and lysine analogues in high-risk cardiac surgery. NEJM 2008;358(22):2319-2331.
- Hebert PC, Fergusson DA, Hutton B, et al. Regulatory decisions pertaining to aprotinin may be putting patients at risk. CMAJ 2014;186(18):1379-1386.
- Faraoni D. Commentary: epsilon-aminocaproic acid versus tranexamic acid, the David and Goliath of antifibrinolytics. JTCVS Open 2020;3:126-127.
- Broadwin MS, Grant PE, Robich MP, et al. Comparison of intraoperative tranexamic acid and epsilon aminocaproic acid in cardiopulmonary bypass patients. JTCVS Open 2020;3:114-125.
- WHO. Executive summary: the selection and use of essential medicines 2019. 2019. Accessed September 2, 2025. https://list.essentialmeds.org/.
- Myles PS, Smith JA, Forbes A, et al. Tranexamic acid in patients undergoing coronary-artery surgery. N Engl J Med 2017;376:136-48.
- Makhija N, Sarupria A, Kumar Choudhary S, et al. Comparison of epsilon aminocaproic acid and tranexamic acid in thoracic aortic surgery: clinical efficacy and safety. J Cardiothorac Vasc Anesth 2013;27(6):1201-1207.
- Tibi P, McClure RS, Huang J, et al. STS/SCA/AmSECT/SABM update to the clinical practice guidelines on patient blood management. Ann Thorac Surg 2021;112:981–1004.
- Wang E, Yuan X, Wang Y, et al. Tranexamic acid administered during off-pump coronary artery bypass graft surgeries achieves good safety effects and hemostasis. Front Cardiovasc Med 2022;9:775760.
- Jerath A, Yang QJ, Pang KS, et al. Tranexamic acid dosing for cardiac surgical patients with chronic renal dysfunction: a new dosing regimen. Anesth Analg 2018;127(6):1323-1332.
- Guo J, Gao X, Ma Y, et al. Different dose regimes and administration methods of tranexamic acid in cardiac surgery: a meta-analysis of randomized trials. BMC Anesthesiol 2019;19(1):129.
- Shi J, Zhou C, Pan W, et al. Effect of high- vs low-dose tranexamic acid infusion on need for red blood cell transfusion and adverse events in patients undergoing cardiac surgery: the OPTIMAL randomized clinical trial. JAMA 2022;328(4):336-347.
- Shakur H, Roberts I, Bautista R, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet 2010;376:23-32.
- Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess 2013;17(10):1-79.
- Morrison JJ, Dubose JJ, Rasmussen TE, et al. Military application of tranexamic acid in trauma emergency resuscitation (MATTERs) study. Arc Surg 2012;147(2)113-119.
- Almuwallad A, Cole E, Ross J, et al. The impact of prehospital TXA on mortality among bleeding trauma patients: a systematic review and meta-analysis. J Trauma Acute Care Surg 2021;90:901-907.
- The PATCH-Trauma Investigators and the ANZICS Clinical Trials Group. Prehospital tranexamic acid for severe trauma. New Engl J Med 2023;389(2):127-136.
- Houston BL, Fergusson DA, Falk J, et al. Prophylactic tranexamic acid use in non-cardiac surgeries at high risk for transfusion. Transfus Med 2021;31:236-242.
- Fillingham YA, Ramkumar DB, Jevsevar DS, et al. Tranexamic acid in total joint arthroplasty: the endorsed clinical practice guides of the American Association of Hip and Knee Surgeons, American Society of Regional Anesthesia and Pain Medicine, American Academy of Orthopaedic Surgeons, Hip Society, and Knee Society. Reg Anesth Pain Med 2019;44(1):7-11.
- Fillingham YA, Ramkumar DB, Jevsevar DS, et al. The efficacy of tranexamic acid in total knee arthroplasty: a network meta-analysis. J Arthroplasty 2018;33(10):3090-3098.
- Dong Q, Zhang Y, Sun X, et al. The effectiveness and safety of aminocaproic acid for reducing blood loss in total knee and hip arthroplasty: a meta-analysis. Int J Surg 2018;52:156-163.
- Zak SG, Tang A, Sharan M, et al. Tranexamic acid is safe in patients with a history of coronary artery disease undergoing total joint arthroplasty. J Bone Joint Surg Am 2021;103(10):900-904.
- Pacheco LD, Saade GR, Hankins GDV. Medical management of postpartum hemorrhage an update. Semin Perinatol 2019;43(1):22-26.
- Shakur H, Roberts I, Chaudri R, et al. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet 2017;389:2105-2116.
- Sentilhes L, Winer N, Azria E, et al. Tranexamic acid for the prevention of blood loss after vaginal delivery. N Engl J Med 2018;379:731-742.
- Sentilhes L, Senat MV, Le Lous M, et al. Tranexamic acid for the prevention of blood loss after cesarean delivery. N Engl J Med 2021;384:1623-1634.
- Pacheco LD, Clifton RG, Saade GR, et al. Tranexamic acid to prevent obstetrical hemorrhage after cesarean delivery. N Engl J Med 2023;388:1365-1375.
- Devereaux PJ, Marcucci M, Painter TW, et al. Tranexamic acid in patients undergoing noncardiac surgery. N Engl J Med 2022;386:1986-1997.
|