|
 Overview | Understanding Coagulation | Assessment & Monitoring | Clinical Contexts | Treatment Strategies | Reversal of Anticoagulation & Antiplatelets | Guidelines & Evidence Overview | Understanding Coagulation | Assessment & Monitoring | Clinical Contexts | Treatment Strategies | Reversal of Anticoagulation & Antiplatelets | Guidelines & Evidence
Laboratory Monitoring of Coagulopathy
Contributed by: Majed Refaai, MD

What is Coagulopathy?
The fibrinolytic system is a necessary component of our hemostatic mechanism which is required to maintain vascular patency. Fibrinolysis remains in balance with coagulation to prevent excessive clot growth by breaking down fibrin. This process first involves the activation of plasminogen (produced in the liver) to plasmin by tissue plasminogen activator (released from injured tissues). Plasmin can then act directly on fibrin to break it down into fibrin degradation products.1 The balance between coagulation and fibrinolysis can shift towards excessive fibrinolysis after certain situations such as trauma or surgery, resulting in excessive bleeding.
Coagulopathy is a medical condition characterized by the impaired ability to maintain normal hemostasis in blood circulation, which increases the risk of excessive bleeding or thrombosis. This complex disorder can result from various factors, including genetic predispositions, liver dysfunction, medications (such as anticoagulants), and other underlying health conditions. Diagnosis usually involves comprehensive blood tests to evaluate the activity of clotting factors, fibrinogen, and platelet function, providing a clear understanding of the individual’s hemostatic status. Management of coagulopathy is tailored to address the underlying causes and may include approaches from adjusting medications to implementing specific therapies aimed at managing both bleeding and clotting risks. Understanding coagulopathy is crucial for all medical professionals working to restore hemostatic balance.
Monitoring of Coagulopathy
Monitoring of coagulopathy is a vital process that ensures the delicate balance of the hemostatic system is maintained, safeguarding patients from the risks of excessive bleeding or clotting. This involves a series of assessments to evaluate the hemostatic system's function and identify any abnormalities in blood coagulation. It is crucial in various clinical settings, especially in patients with liver disease, those undergoing anticoagulant therapy, or those who have undergone major surgeries. Key elements in the monitoring process include:
- Clinical Evaluation: A meticulous assessment of the patient’s medical history, along with keen observation for any signs of bleeding or clotting disorders, forms the cornerstone of effective monitoring.
- Laboratory Tests: A suite of tests helps illuminate the intricacies of blood coagulation. These tests evaluate various aspects of the coagulation process, helping to identify abnormalities that can lead to excessive bleeding or thrombotic conditions.
- Point-of-Care Testing: In urgent situations, point-of-care testing devices are utilized for immediate results, especially in emergency settings, empowering clinicians to make timely and informed decisions.
- Management: With the insights gained from monitoring, tailored interventions can be implemented, such as adjusting anticoagulant dosages, utilizing clotting factor concentrates, or proactively addressing potential bleeding risks. Continual monitoring is essential to ensure patient safety and effective management of coagulopathy, adapting interventions as necessary based on test results and clinical judgment.
Coagulopathy Tests
Coagulopathy tests are vital tools in the realm of medicine, playing a crucial role in the diagnosis and management of blood clotting disorders. By intricately evaluating various facets of the coagulation process, these tests illuminate underlying abnormalities that can lead to either excessive bleeding or potentially dangerous thrombotic conditions. Here are some of the key tests that form the backbone of coagulopathy assessment: Prothrombin Time (PT) and Activated Partial Thromboplastin Time (aPTT) which provide insight into the functionality of the extrinsic and intrinsic coagulation factors, respectively; International Normalized Ratio (INR) for those on vitamin K antagonist (VKA) anticoagulation therapy; Platelet Count; Fibrinogen Levels; Thrombin Time; and D-Dimer, which detects the presence of fibrin degradation products.
In addition, more special coagulation tests can be performed, such as Coagulation Factor Assays that may identify deficiencies or abnormalities in specific coagulation pathways. Together, these tests provide valuable information to guide further investigation and treatment plans. However, interpreting these results requires a holistic view, considering the patient’s clinical history and findings.
Viscoelastic Tests in Coagulopathy
Unlike traditional coagulation tests, which typically measure individual components of the clotting cascade, viscoelastic tests provide a more comprehensive assessment of coagulopathies by revealing specific clotting abnormalities. In these tests, a fresh whole blood sample is subjected to conditions that mimic physiological clotting, and various measurements are taken throughout the clotting process to evaluate different kinetic parameters. Each parameter offers insights into various aspects of hemostasis, such as deficiencies in clotting factors, platelet dysfunction, or imbalances in the fibrinolytic pathway. This information aids in identifying specific coagulopathy issues and informs treatment decisions. The quick results from viscoelastic tests enable immediate clinical decision-making, especially in critical care settings where timely interventions can significantly affect patient outcomes.
Additionally, viscoelastic tests can guide transfusion practices by helping clinicians determine when and what type of coagulation factor replacement or platelet transfusion is necessary, thus avoiding unnecessary or excessive treatments.
Examples of Coagulopathy
Coagulopathy disorders embody a range of conditions that impact clot formation. Here are some noteworthy examples:
- Hemophilia: A hereditary condition that impedes the clotting process due to the absence or deficiencies of specific clotting factors, particularly factor VIII (Hemophilia A) or factor IX (Hemophilia B).
- Von Willebrand Disease: the most prevalent inherited bleeding disorder caused by a deficiency or dysfunction of von Willebrand factor, which aids platelets adhesion to the injured blood vessel wall and is also a carrier for clotting factor VIII.
- Liver Disease: Conditions affecting the liver, such as cirrhosis or hepatitis, can impair the production of clotting factors, leading to coagulopathy.
- Vitamin K Deficiency: Vitamin K is essential for the synthesis of several key clotting factors. Insufficient vitamin K due to poor diet or malabsorption can provoke bleeding diathesis.
- Disseminated Intravascular Coagulation (DIC): A complex and serious condition that is often triggered by a systemic inflammatory response or the release of procoagulants into the bloodstream. This lead to the activation of the coagulation cascade, resulting in the formation of small blood clots throughout the circulatory system, leading to organ dysfunction and life-threatening bleeding. Many conditions can lead to DIC including sepsis, trauma, burns, cancer, and pancreatitis.
- Antiphospholipid Syndrome: An autoimmune disorder where antibodies against certain phospholipids are formed causing cell activation and elevating the risk of clot formation.
- Factor V Leiden: A thrombotic disorder due to a genetic mutation of the coagulation factor V increases the propensity for blood clots by rendering the blood resistant to activated protein C, a crucial regulator in the coagulation pathway.
- Acquired Coagulopathy: Arising from various factors such as certain medications (like anticoagulants), malignancies, or other underlying diseases, acquired coagulopathy further complicates the landscape of blood clotting disorders.
Understanding these diverse coagulopathy disorders is essential for effectively managing potential complications and ensuring optimal outcomes. By shedding light on these conditions, clinicians can foster better awareness and improve the quality of care.
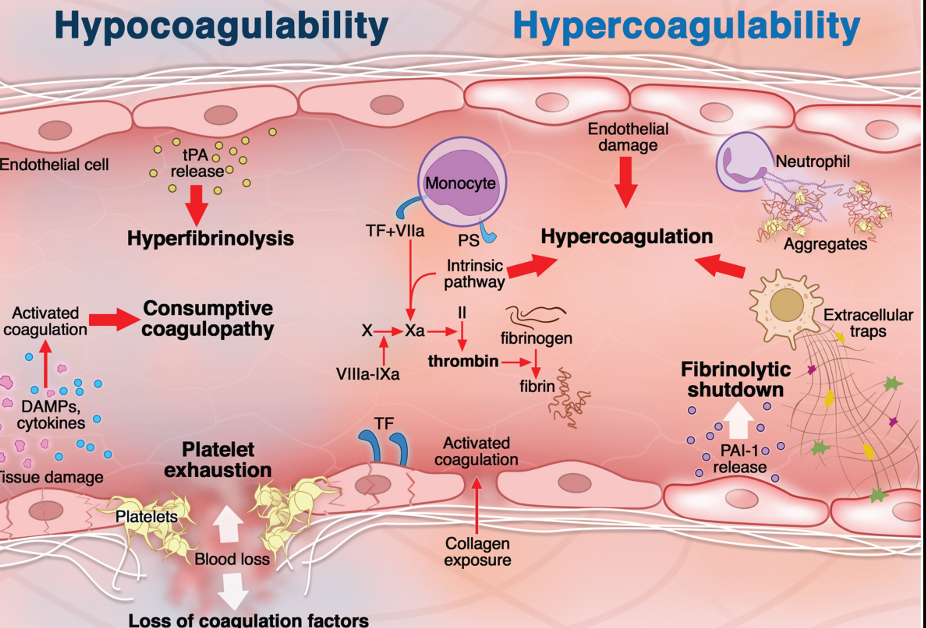
Helms, J., Iba, T., Connors, J.M. et al. How to manage coagulopathies in critically ill patients. Intensive Care Med 49, 273–290 (2023). https://doi.org/10.1007/s00134-023-06980-6
References
- Savi M, Hawryluk G. Thrombosis and Coagulopathy. Neurosurg Clin N Am. 2025;36(3):375-385.
- Lindsay C, Davenport R, Baksaas-Aasen K, et al. Correction of Trauma-induced Coagulopathy by Goal-directed Therapy: A Secondary Analysis of the ITACTIC Trial. Anesthesiology. 2024;141(5):904-912.
- Iba T, Levy JH. Sepsis-induced Coagulopathy and Disseminated Intravascular Coagulation. Anesthesiology. 2020;132(5):1238-1245.
- Singh AD, Mucha SR, Lindenmeyer CC. Cirrhotic coagulopathy: A rebalanced hemostasis. Cleve Clin J Med. 2022;89(9):523-533.
- Iba T, Helms J, Neal MD, Levy JH. Mechanisms and management of the coagulopathy of trauma and sepsis: trauma-induced coagulopathy, sepsis-induced coagulopathy, and disseminated intravascular coagulation. J Thromb Haemost. 2023;21(12):3360-3370.
- Maier CL, Brohi K, Curry N, et al. Contemporary management of major haemorrhage in critical care. Intensive Care Med. 2024;50(3):319-331.
- Giustozzi M, Ehrlinder H, Bongiovanni D, et al. Coagulopathy and sepsis: Pathophysiology, clinical manifestations and treatment. Blood Rev. 2021;50:100864.
|