Coagulopathy can be caused by congenital or acquired platelet or factor deficiencies. Acquired deficiencies can be due to various medications, due to interruption in platelet function, or interruption in the coagulation cascade. When medication-induced coagulopathy occurs, it is vital to know the offending agent if possible, various tools to measure or assess the degree or coagulopathy or dysfunction, and options for correcting the coagulopathy.
Antiplatelets
Antiplatelet agents are used for various medical reasons, such as reduction in cardiovascular disease and stroke (1). The main anti-platelet agents encountered are aspirin and the class of medications known as P2Y12 inhibitors.
Aspirin
Mechanism of Action
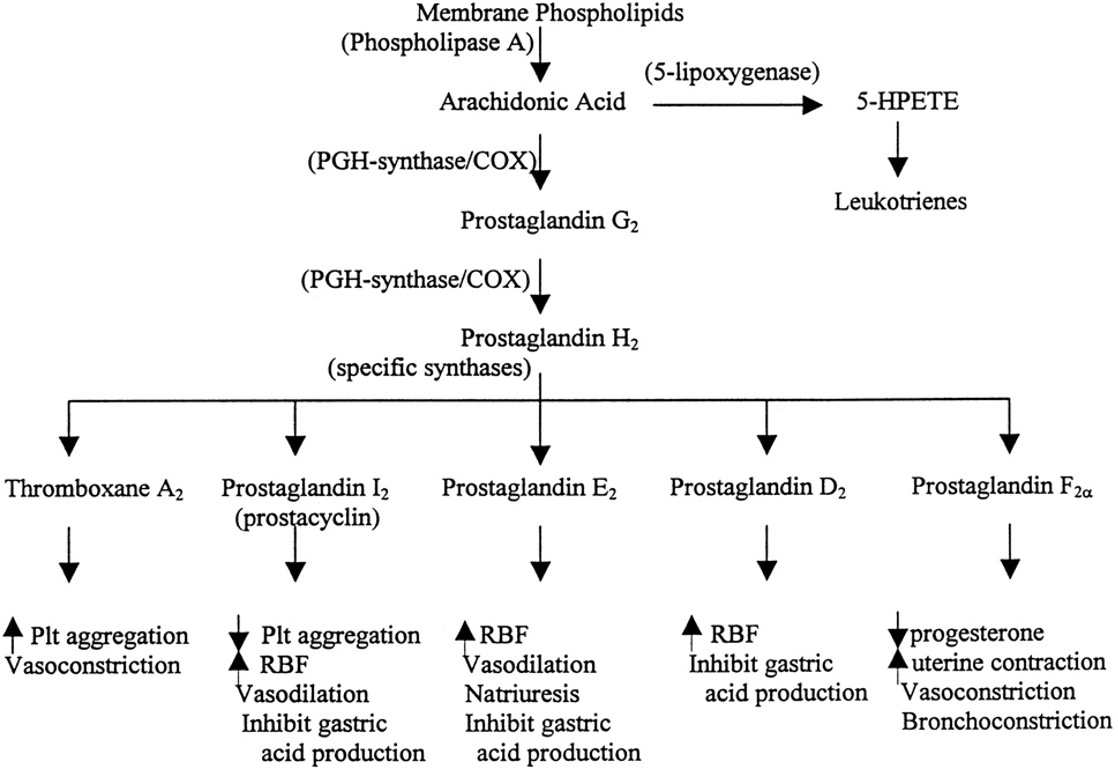
Aspirin exerts its effect primarily by interfering with the biosynthesis of cyclic prostanoids, ie, thromboxane A2 (TXA2), prostacyclin, and other prostaglandins (2).
Testing
Testing for aspirin effect includes platelet function assays.
- Options include Thromboelastography-platelet mapping (TEG-PM), platelet mapping, and VerifyNow (reports platelet functions in terms of aspirin-reaction units (ARU)).
- TEG Platelet Mapping Assay is able to provide a semiquantitative analysis of platelet function through evaluation of the contribution of the ADP or thromboxane A2 (TxA2) receptors.
- VerifyNow was created to determine if patients taking aspirin had adequate platelet inhibition, and therefore were not aspirin resistant. Although this test was created to evaluate aspirin resistance and compliance, this test has been used pre-operatively to determine bleeding risk as well (11).
Treatment
Aspirin irreversibly inhibits cyclooxygenase, and therefore there is no reversal agent. The minimum time from drug interruption to platelet restoration is 4 days (4). Treatment would therefore include support care and transfusion of platelets to aid in hemostasis.
P2Y12 Inhibitors
Mechanism of Action
P2Y12 inhibitors work by binding to the P2Y12 receptor on platelets, and therefore prevent activation and aggregation. P2Y12 inhibitors may be used as dual anti-platelet therapy along with aspirin in patients with acute coronary syndromes or those who undergo percutaneous coronary intervention.
Medications
The medications within the class of P2Y12 inhibitors include clopidogrel, ticagrelor, prasugrel and cangrelor (3).
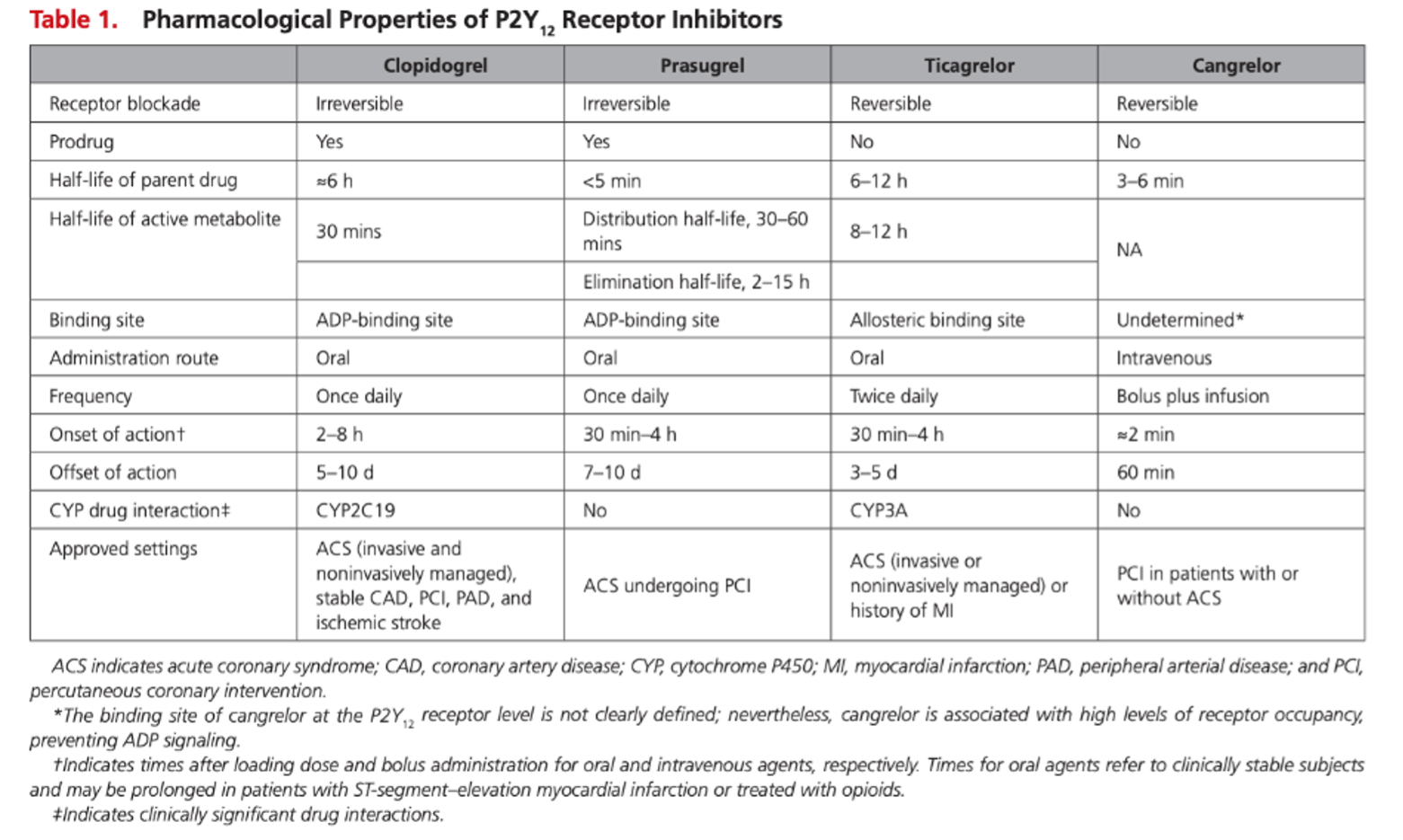
- Clopidogrel is a prodrug and therefore must be metabolized to its active form to work.
- Cangrelor is unique as it is an intravenous P2Y12 inhibitor, with a rapid onset and offset of approximately 3 minutes. The rapid off-set is due to metabolism of the medication by plasma esterases, which makes it a useful anti-platelet agent medication in those who are at high risk of bleeding or in need or procedures or surgeries.
Testing
Similar to aspirin, platelet function assays can be utilized to assess for responsiveness or nonadherence to P2Y12 inhibitors. Additionally, platelet function testing may help determine timing of surgery following withdrawal of P2Y12 inhibitors, such as for cardiac surgery. TEG-PM and VerifyNow may be used.
Example of TEG-PM:
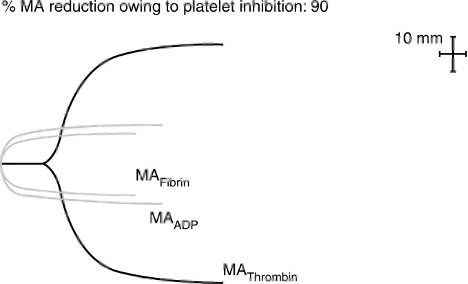
This is a patient with 90% inhibition, who was recently on clopidogrel.
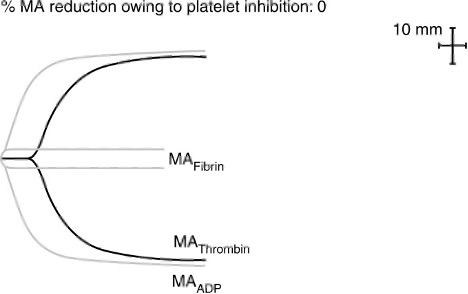
This is a patient who was not taking any anti-platelets, with 0% inhibition (13).
VerifyNow may be used, and reports in terms of P2Y12 reaction units (PRU)
- Low response or nonresponse is indicated by high platelet reactivity.
Guidelines for Cessation Prior to Surgery or Procedures
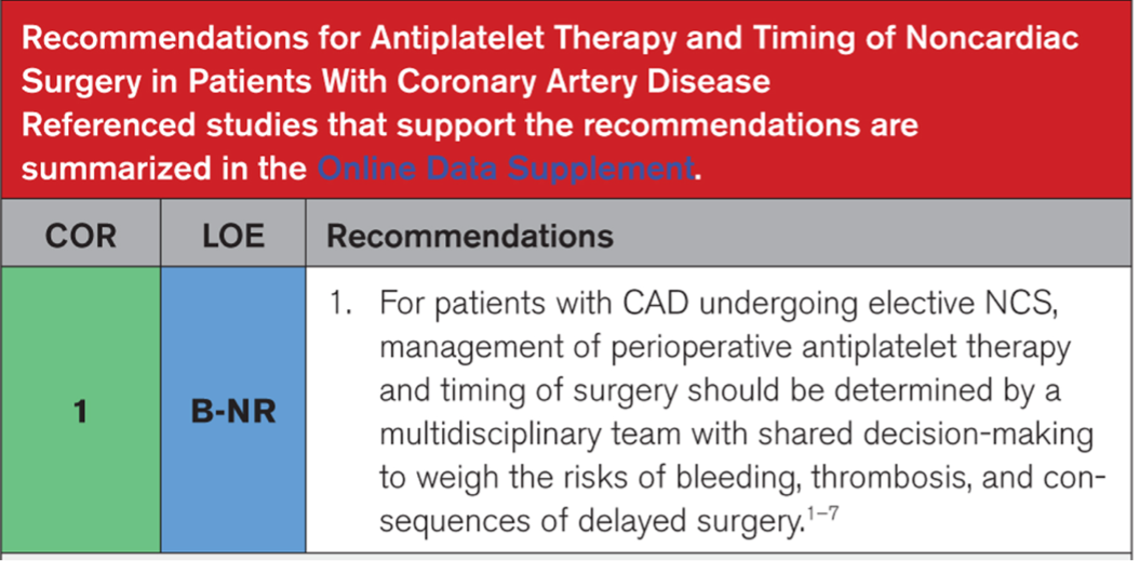
When anticipating invasive procedures or surgeries, P2Y12 inhibitors need to be held to minimize bleeding risks. The 2024 ACC/AHA guidelines recommend the management of anti-platelet therapy be determined by a multi-disciplinary team to weigh the risks of bleeding, thrombosis, and consequences of delay of surgery (4).
Treatment
Supportive care with cessation of the medication and platelet transfusions may be necessary if a bleeding patient was on a P2Y12 inhibitor.
Anticoagulants
Anticoagulants are varying classes of medications that are used to prevent or treat thrombosis. Vitamin K antagonists were the traditional medications used, followed by direct oral anticoagulants. These medications may be used in situations such as atrial fibrillation for stroke prevention, treatment or prevention of venous thromboembolism, or other states in which there is a high risk of thrombosis.
Vitamin K Antagonists (VKA)
Mechanism of Action
VKAs work by inhibiting the enzyme vitamin K epoxide reductase, and therefore prevent the synthesis of vitamin K dependent clotting factors, such as factors II, VII, IX, and X.
Medications
Warfarin is the most commonly used oral VKA.
Testing
International normalized ratio (INR) is used to determine the effect of VKAs. Elevated INR levels have been associated with bleeding.
Guidelines for cessation prior to surgery or procedures
VKAs should be held for 5 days prior to surgery or an invasive procedure (4). In patients with high thromboembolic risks, bridging with heparin may be utilized.
Treatment
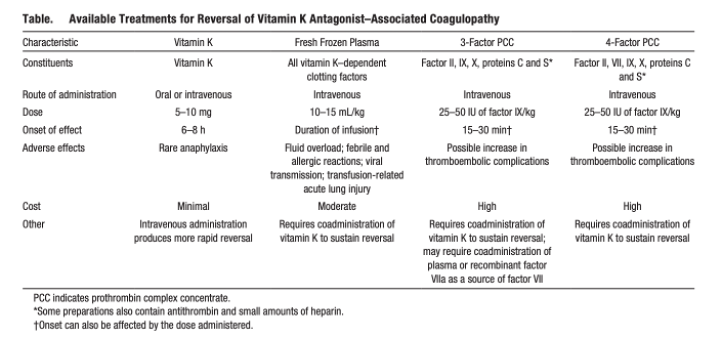
Treatment options include vitamin K supplementation, prothrombin complex concentrates (PCCs), and plasma administration.
- Vitamin K Supplementation
- Vitamin K reverses the effects of VKAs. In bleeding patients, or prior to surgery or an invasive procedure, IV vitamin K may be given. The onset is approximately 2 hours. Subcutaneous vitamin K can also be given, but its absorption and response is less predictable.
- In non-bleeding patients with an elevated INR of 4.5-10, the recommendation is not to administered vitamin K to these patients. A 2019 systematic review supported this recommendation (5).
- Prothrombin complex concentrates (PCCs)
- PCCs include 3-factor (3F), 4-factor (4F), or activated PCCs. 3F-PCCs include factors II, IX,and X, 4F-PCCs include II, VII, IX, and X, and aPCCs include II, IX, X, and activated VII.
- Sarode et al (6) found that 4F-PCC were noninferior to plasma in terms of efficacy, and superior with respect to safety. Guidelines therefore support 4F-PCC over plasma in bleeding patients taking VKAs.
- PCCs have several advantages to plasma including faster reversal, no need for blood matching, reduced viral transmission, and reduced risk of volume overload.
- Plasma
- Plasma contains clotting factors amongst others components, and can also therefore reverse the effects of VKAs.
Direct Oral Anticoagulants (DOACs)
Mechanism of Action
DOACs are classified into two major categories based on mechanism of action. Direct thrombin inhibitors (DTIs) are one class, and Xa inhibitors are another class.
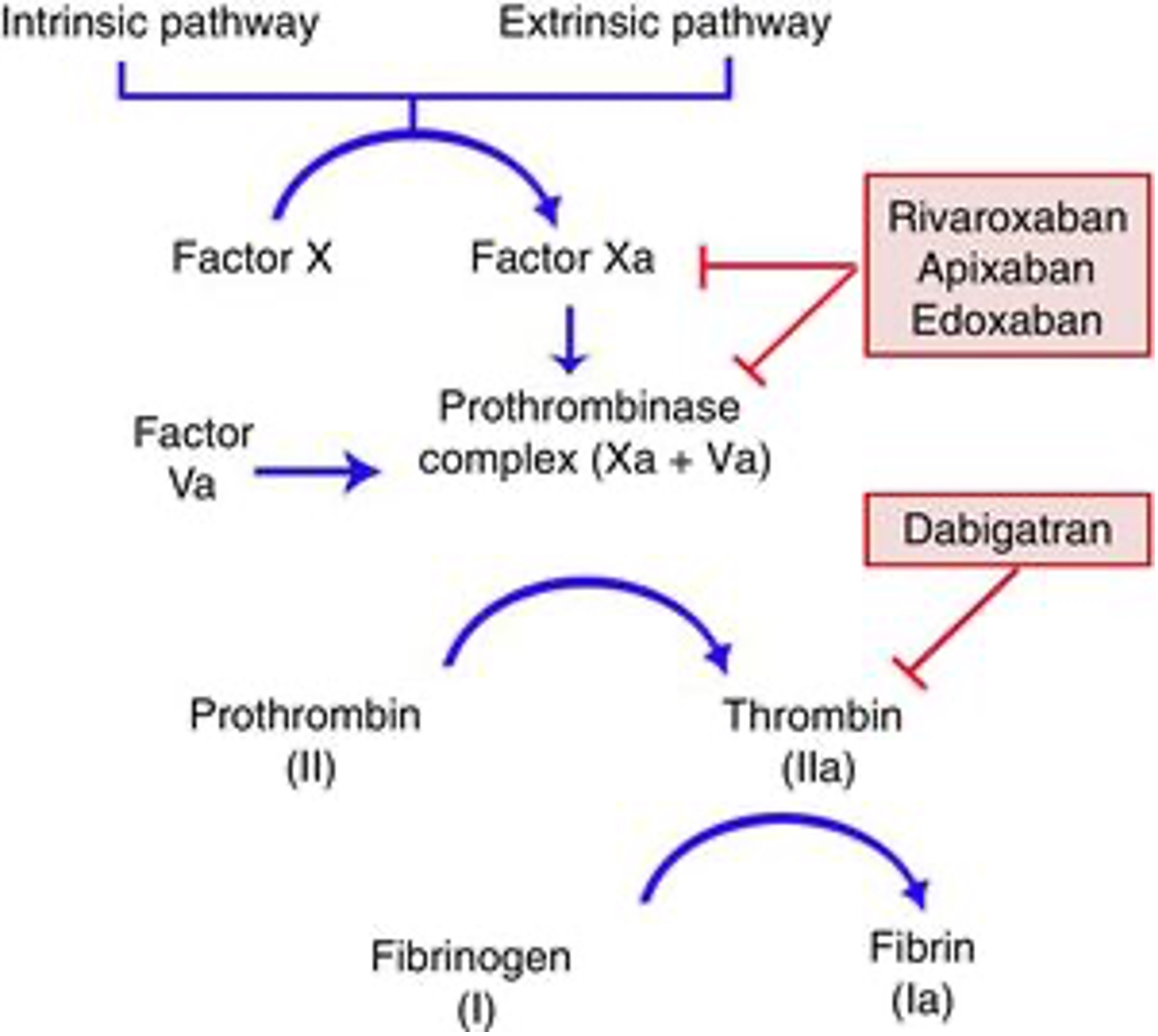
Medications
- DTIs include the oral agent, dabigatran, and intravenous agents, argatroban and bivalrudin.
- Xa Inhibitors include the oral agents apixaban, rivaroxaban, and edoxaban.
- XI inhibitors are emerging as potential anticoagulants with the same goal of preventing thromboembolism while minimizing bleeding risks.
Testing
- Global coagulation testing (such as prothrombin time (PT) and activated partial thromboplastin time (aPTT)) has not been proven to be beneficial in assessing the coagulant effect of DOACs; and therefore, are not recommended to assess relevant DOAC concentrations.
- The one exception is using dilute thrombin time for dabigatran, where a normal thrombin time represents no residual dabigatran effect.
- Drug-specific calibrated anti-Xa assays are regarded as the “gold standard” method for monitoring direct anti-Xa inhibitors. If drug-specific anti-Xa assays are not available, chromogenic anti-Xa assays calibrated for unfractionated heparin can be utilized with sufficient accuracy.
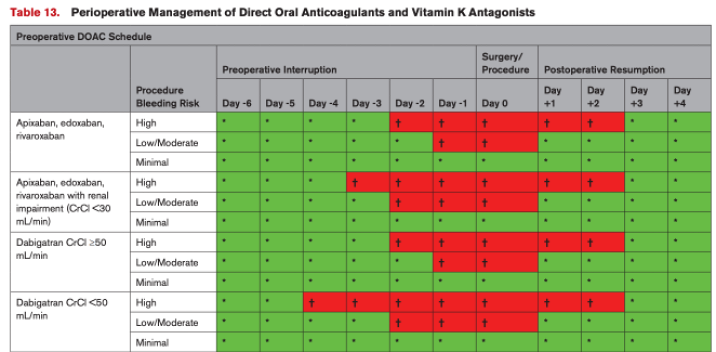
Guidelines for Cessation Prior to Surgery or Procedures
The 2024 ACC/AHA guidelines recommend the management of oral anticoagulants be determined by a multi-disciplinary team with time-based interruption to balance the competing risks of thromboembolism and bleeding (4).
Treatment
- Treatment options include PCCs, plasma, or direct reversal agents. For rivaroxaban and apixaban, andexanet alfa is a Xa decoy molecule that binds the medication making it relatively inactive in a matter a minutes. The Anexxa-4 trial (9) looked at patients taking Xa inhibitors with major bleeds, majority were gastrointestinal and intracranial hemorrhages. Xa activity level decreased by 89% and 93% in patients taking rivaroxaban and apixaban respectively. Additionally, hemostasis was excellent or good in 79% of patients, with thrombotic events occurring in 18% of patients at a 30-day follow-up. This to approval of andexanet alfa for major bleeding associated with rivaroxaban or apixaban.
- The Anexxa-I was a follow-up trial looking solely at patients with intra-cranial hemorrhage who were taking Xa inhibitors. Patients either received andexanet alfa, or usual care. The patients who received andexanet alfa 67% had hemostatic efficacy compared to 53.1% in the usual carer group. Additionally, Xa activity level decreased 94.5% in the andexanet group compared to 26.9% in the usual care group. Thrombotic events occurred in 10.3% in the andexanet group compared to 5.6% in the usual care group. Of note, 85.5% of patients in the usual care group received PCCs.
- Although andexanet alfa has been used in major bleeding with good results, the use in cardiac surgery should be carefully considered as many case reports and series document inability to appropriate heparinize for cardiopulmonary bypass or even the formation pump thrombosis. Therefore, this specific population has many risks associated with andexanet alfa use.
- Idarucizumab is an antibody fragment and directly reverses the effect of dabigatran within minutes (12).
References
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646
- Awtry, EH, Loscalzo, J. Aspirin. Circulation. 2000;101(10)
- Angiolillo DJ, Rollini F, Storey RF, Bhatt DL, James S, et al. International Expert Consensus on Switching Platelet P2Y12 Receptor-Inhibiting Therapies. Circulation. 2017;136(20).
- Thompson A, Fleischmann KE, Smilowitz NR, de las Fuentes L, Mukherjee D, et al. 2024 AHA/ACC/ACS/ASNC/HRS/SCA/SCCT/SCMR/SVM Guideline for Perioperative Cardiovascular Management for Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;15(19)
- Khatib R, Ludwikowska M, Witt DM, Ansell J, Clark NP, et al. Vitamin K for reversal of excessive vitamin K antagonist anticoagulation: a systematic reviewe and meta-analysis. Blood Adv. 2019;3(5):789-796
- Sarode R, Milling TJ Jr, Refaai MA, et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized